Frequently young patients come to me asking for a tooth to be removed, because their teeth are bad. But are they really bad and is removing the tooth the best way to go?
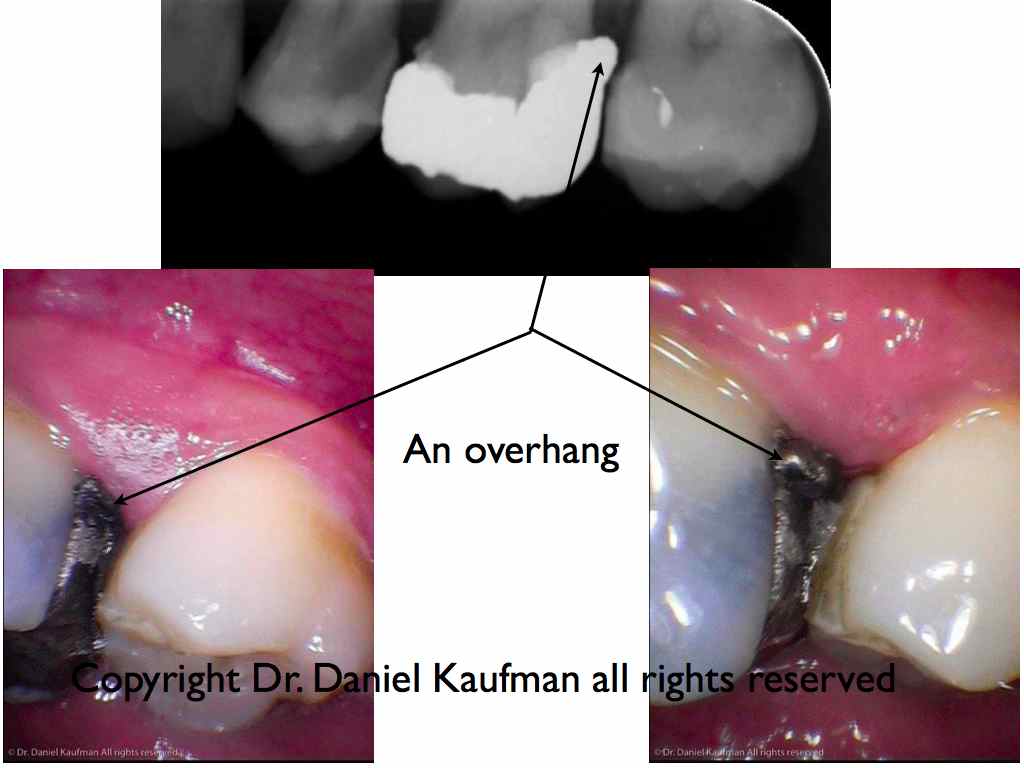
The broken down teeth are usually consequences of two common diseases. The first is decay, which is a bacterial assault on our teeth fueled by sugars from our die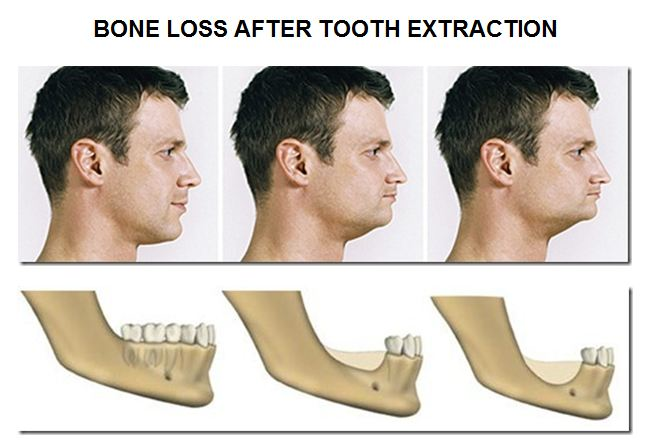 t. The second is gum disease caused by bacteria colonizing the soft tissue around the teeth and making an infection there which can penetrate further to the bone, blood system and from there to the whole body. These problems are caused by bacteria and their removal will sort things out.
t. The second is gum disease caused by bacteria colonizing the soft tissue around the teeth and making an infection there which can penetrate further to the bone, blood system and from there to the whole body. These problems are caused by bacteria and their removal will sort things out.
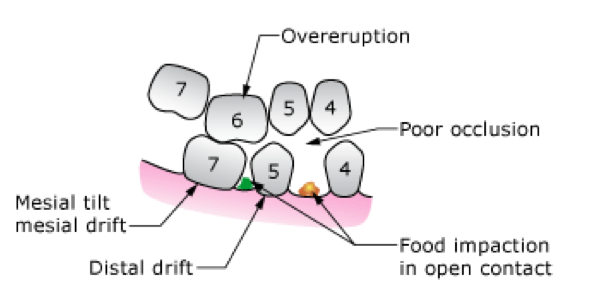
So there are no bad teeth, removing the bacteria and dealing with the causes to tooth break down will keep them in your mouth. Having the teeth removed will only make things worse for the remaining ones, by overloading them, leading them to move and make chewing difficult. Once the teeth are removed, the bone that surrounds the them will go leading to changes in your appearance that make you look older.
Please come and see us to keep your teeth.